Brain Tumors
GliomasGliomas are a group of most probably malignant tumors that can arise anywhere in the central nervous system (CNS), that is, in the brain or less commonly, in the spinal cord. These tumors are characterized by an infiltrative growth pattern and/or a tendency to spread locally into the CNS. Expansion of the tumor outside the brain usually does not occur.
After histopathological examination, gliomas are generally named according to the type of nerve cells from which they derive (astrocytes, oligodendrocytes or ependymal cells). The classification of gliomas is carried out on a scale of I to IV (1 to 4) which reflects the growth rate of the tumor as well as its aggressiveness. Grade I tumors, which mainly occur during childhood, are associated with the best prognosis. Grade II (low-grade gliomas) characterize slow-growing, infiltrating tumours, with an intermediate prognosis. On the other hand, grade III (anaplastic) and grade IV (glioblastoma) tumors are considered high-grade gliomas because they are aggressive and generally have a less favorable prognosis.
Main glioma types:
- Grade II oligodendrogliomas
- Anaplastic oligodendrogliomas (also called grade III)
- Grade II astrocytomas
- Anaplastic astrocytomas (also called grade III)
- Glioblastomas (also called grade IV)
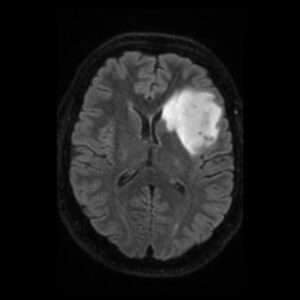
You can find below an MRI image of a low-grade glioma:
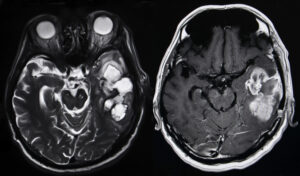
And here you can find an MRI image of a glioblastoma (a grade IV glioma):
Treatment
Surgery
Regardless of glioma subtype, surgery (surgical resection or stereotactic/open biopsy) is an essential part of treatment for all newly diagnosed gliomas.
Surgical resection
Surgical resection of the tumor is the recommended initial treatment for the majority of gliomas. The surgery aims to be as complete as possible. This is motivated by the demonstration that maximum tumor resection results in longer survival and allows for more effective postoperative treatments. But if such a radical surgery risks altering neurological functions, it must aim to remove as much of the tumor as possible while sparing healthy tissue.
In addition, surgical removal of the tumor should provide sufficient tissue for accurate histopathological diagnosis and molecular characterization of the tumor.
Stereotaxic/open biopsy
If surgery is impossible safely, in particular because of the location of the tumor (for example, in an area that is inaccessible surgically or at high risk of significant impairment of neurological functions) or a deteriorated clinical condition, stereotaxic or open biopsy to remove tissue for diagnosis may be considered. The biopsy does not treat the tumor, but the analysis of the tissues removed by biopsy makes it possible to establish the best treatment. A stereotactic biopsy is the least invasive way to take a tissue sample, while an open biopsy is a surgical procedure using local or general anesthesia to remove the tissue needed for diagnosis. Performed by an experienced physician, a stereotaxic biopsy provides enough tissue to establish a correct histopathological diagnosis in more than 95% of cases. However, to provide as much tissue as possible for diagnosis and molecular characterization, open biopsy remains preferable.
Radiotherapy and/or chemotherapy
Postoperative treatments mainly consist of chemotherapy and/or radiotherapy. However, their implementation depends on the glioma subtype. A simple observation can be also adopted after surgery, if surgery succeeded to remove all or the majority of the tumor and histopathological examination showed non agressive tumor.
Radiatherapy usually follows surgery in treatment of glioma, especially high-grade gliomas. Radiation uses high-energy beams, such as X-rays or protons, to kill tumor cells left after surgical treatment. Radiotherapy for glioma is done by a machine outside the body by external beam radiation. Side effects of radiatherapy depend on the type and dose of radiation you receive. Common side effects during or immediately following radiation include fatigue, headaches and scalp irritation. There is also long term side effects, as cognitive decline or memory disorders.

Chemotherapy uses drugs to kill tumor cells. These drugs can be given in pill form (orally) or injected in a vein (intravenously). Chemotherapy is usually used in combination with radiotherapy to treat gliomas. The most often used chemotherapy drug to treat gliomas is temozolomide (Temodal), which is given orally. Side effects of chemotherapy depend on the type and dose of drugs used. Common side effects include nausea and vomiting, headache, hair loss, fever, and weakness. Some side effects may be managed with medication. Chemotherapy can be interrupted if there is more severe side effects.